CRISPR-Armed Phages Clear First Human Safety Bar
CMN Interview
Mar. 3, 2026


CMN Intelligence - The World’s Most Comprehensive Intelligence Platform for CRISPR-Genomic Medicine and Gene-Editing Clinical Development
Providing market intelligence, data infrastructure, analytics, and reporting services for the global gene-editing sector. Read more...

August was born about seven years ago. On the website ‘Sammen for August’, he appears as a cheerful boy surrounded by a loving family. Early on, however, his parents, Tina and Søren, noticed that August’s development was not keeping pace with expectations. This led to a series of medical examinations that revealed unexplained damage to his central nervous system. A four-year diagnostic odyssey finally came to an end when comprehensive genetic testing showed that August carried biallelic mutations in the AP4M1 gene, the cause of an ultra-rare, progressive neurodegenerative disorder known as Hereditary Spastic Paraplegia type 50 (SPG50).
»There are only about 100 children diagnosed with SPG50 worldwide,« explains August’s father, Søren Jarl Christensen. »When our son was diagnosed in 2022, we were told there was no treatment. The doctors said we should just enjoy the time we had with him. We went home completely devastated.«
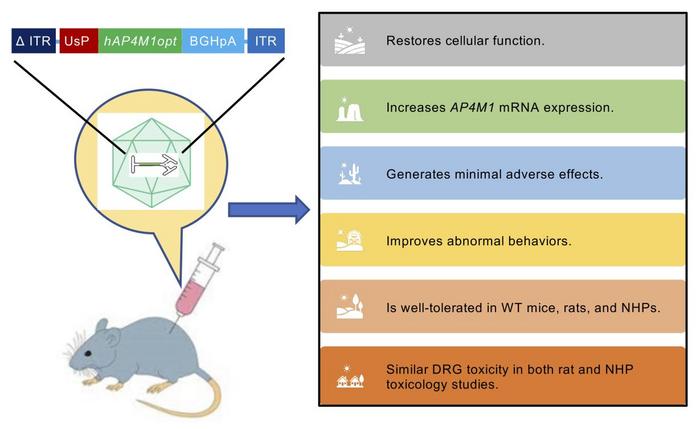
That changed in early 2023, when the family learned that Terry Pirovolakis, a parent of a child with SPG50 in Canada, had organized the development of ‘Melpida’, an investigational gene replacement therapy. Melpida uses an adeno-associated virus serotype 9 (AAV9) vector to deliver a functional AP4M1 gene to neurons via cerebrospinal fluid. 1 The therapy had received authorisation from Canadian and U.S. regulatory authorities to enter clinical development, and early clinical programs were initiated in Toronto and Dallas, Texas. 2
»There are only about 100 children diagnosed with SPG50 worldwide,« explains August’s father, Søren Jarl Christensen. »When our son was diagnosed in 2022, we were told there was no treatment. The doctors said we should just enjoy the time we had with him. We went home completely devastated.«
That changed in early 2023, when the family learned that Terry Pirovolakis, a parent of a child with SPG50 in Canada, had organized the development of ‘Melpida’, an investigational gene replacement therapy. Melpida uses an adeno-associated virus serotype 9 (AAV9) vector to deliver a functional AP4M1 gene to neurons via cerebrospinal fluid. 1 The therapy had received authorisation from Canadian and U.S. regulatory authorities to enter clinical development, and early clinical programs were initiated in Toronto and Dallas, Texas. 2
A continuous quest for timely therapeutic access and funding
To better understand August’s disease course, the family travelled to Boston to participate in a natural history study on Hereditary Spastic Paraplegia type 50. In parallel, Søren began reaching out to clinicians, researchers, and patient advocates to secure August a place in a U.S.-based clinical trial.
»We tried everything to get our son into the clinical trial in the United States, but as time passed, he became too old to meet the trial’s selection criteria. With a progressive disease, time is everything, another delay of treatment means more functional decline, something you don’t get back.«
Returning to Denmark, the family faced the harsh realisation that while a promising therapy existed, there was no clear pathway to fund or access it through the national healthcare system. Also, hopes of participating in a future Phase 2 or 3 trial faded when U.S. funding was abruptly cut following political changes.
Elpida Therapeutics offered to support an effort to treat August and a second Danish child by providing personnel, training, and clinical protocols. However, the gene therapy itself, supplied at cost, still amounted to approximately USD 350,000 per treatment, and Søren and his family would need to navigate European regulatory approval largely on their own.

»At that point, there was no other option. We had to create a foundation and start raising money ourselves. That was the only way to keep the hope of treatment alive. And the clock was ticking for August.«
The family launched national fundraising campaigns and built public awareness through Danish media and a television documentary. Yet fundraising proved challenging.
»Fundraising to pay for medical expenses in Denmark is not easy. People expect the healthcare system to take responsibility. For rare diseases, that expectation leaves families on their own.«
At the same time, Søren approached the specialized Rigshospitalet medical centre to explore whether the treatment could be administered locally. Initial interest was limited.
“At first, our hospital in Denmark was not interested in treating August with Melpida. They didn’t have the infrastructure or resources to conduct experimental gene therapy studies. I also reached out to my international network to bring AP4M1 gene therapy to Denmark, and I was told that Europe is difficult, very difficult”Søren Jarl Christensen.
After months of discussion, constructive conversations began around feasibility, training, and regulatory requirements. »We already had the protocols and technical support from Elpida Therapeutics,« Søren explains. »The missing piece was not the science, but the system around it.« What followed was a prolonged effort to secure regulatory approvals, align institutional responsibilities, and close persistent funding gaps.
The healthcare paradox: paying for care, not prevention
As Søren Jarl Christensen points out, the medical cost of inaction is rarely acknowledged. For children with SPG50, lifelong supportive care - hospitalisations, assistive technologies, specialized education, and constant supervision - can easily reach several million euros over a lifetime. In contrast, a one-time experimental intervention, even at substantial upfront cost, could dramatically alter both clinical trajectory and long-term societal burden.
»In Denmark there are only five children with SPG50, but over a lifetime they will cost the healthcare system far more in long-term care than a one-time Melpida treatment,« Søren explains. »Early treatment could possibly avoid much of the damage and expenses, yet we are asked to prove that the therapy works before any healthcare costs are covered. For rare, progressive diseases, generating that kind of evidence can take years, and by the time the system is convinced, it is often too late. The disease may have progressed too far.«
Fragmentation across Europe
With the cooperation of Rigshospitalet and Elpida Therapeutics, regulatory documentation was assembled using the U.S. trial dossier as a foundation. Approval was fast-tracked at the European level through the European Medicines Agency. However, Søren notes that even a ‘short’ evaluation period of 100 days is a long time when a progressive disease is involved. An additional national medical authorisation process was still required in Denmark. This involved more regulatory and ethics reviews that revisited many of the same questions already assessed at EU level.
Crucially, the preparation, submission, and management of these regulatory filings, at both European and national level, were financed by August’s family foundation, taking critical funding away from resources to cover actual treatment costs.
“What I hope for is a single European genomic medicine approval that is recognized across countries. Requiring both European and national approvals only adds delays and expenses, and with many rare diseases, time and money is something we simply don’t have.”Søren Jarl Christensen
»At the moment, Elpida Therapeutics is organizing separate clinical sites in Italy, Spain, the UK, and Denmark. The current system is so fragmented, at times it feels hopeless. A therapy approved at the European level should not require a new evaluation in every country. When we looked into treatment in another EU Member State, access was subject to national compassionate-use regulations, which meant cross-border treatment was not an option.«

Rare, but not uncommon
SPG50 is ultra-rare, yet the therapeutic strategies developed for it extend far beyond a single diagnosis. Many hereditary neurodegenerative diseases share common cellular pathways and delivery requirements, meaning that advances made for one condition can often be adapted for others. In this sense, SPG50 is rare in prevalence, but not exceptional in biology.
This platform logic is increasingly reflected in gene therapy development. Elpida Therapeutics, for example, is developing AAV9-based gene replacement therapies for SPG50 alongside other related inherited neurological disorders, using the same viral vector backbone combined with disease-specific genetic payloads. At the manufacturing level, a similar approach is taken by Viralgen, a subsidiary of Bayer AG, which operates as a GMP facility designed to support multiple current and future gene therapies, including Melpida.
»Every time we treat a gene therapy as if it’s entirely new, we start from zero,« Søren says. »But the delivery systems are often the same. If we learned how to reuse what already works, we could help many more families.«
“Health is still too often treated as purely a national responsibility. But to ensure patients have access to new and life-saving medicines, we must act across borders. There is so much we can do better when we work together. Europe has the scientific strength to lead in personalised medicine and gene therapy - and we cannot afford to fall behind”Stine Bosse, Vice Chair, European Parliament Committee on the Environment, Public Health and Food Safety (ENVI)
Looking ahead
After years of uncertainty, the coming months may mark a turning point. If all approvals and logistics remain on track, August is expected to receive treatment at Rigshospitalet in the spring of 2026. Elpida Therapeutics has indicated that two doses of the investigational gene therapy are available, at a combined cost of approximately €950,000. Early clinical observations suggest that disease progression in treated children may be slowing or stabilizing, although established neurological damage cannot be reversed.
For Søren Jarl Christensen, the prospect of treatment shifts the focus from one child’s case to the system that governs access. Years spent navigating regulatory reviews, funding gaps, and institutional hesitation have clarified where the system falters, and why families facing ultra-rare diseases can feel left behind as treatments advance in other countries.
Søren’s continuing efforts align directly with the mission of the European Genomic Medicine Consortium: to unite patients, clinicians, scientists, regulators, industry, and policymakers around shared solutions that enable timely and equitable access to genomic medicine across borders.
»No family should have to push this hard just to reach treatment,« Søren says. »If we can adjust the way these therapies are evaluated and approved in Europe, then it won’t just help August - it will help many others.«
Access to genomic medicine: Turning isolated battles into European pathways
In April 2026, the CRISPR Medicine News Conference (CRISPRMED26) in Copenhagen will mark the launch of the European Genomic Medicine Consortium (EGMEDC), a new non-profit initiative aimed at uniting Europe’s fragmented genomic medicine landscape and accelerating clinical translation.
As genomic therapies move from experimental promise toward clinical reality, Europe faces a fundamental question: are our systems prepared to deliver them to patients in need? For rare diseases, this challenge begins with access to accurate genetic diagnostics and extends across clinical development, regulation, reimbursement, and cross-border care.
August’s journey is not just about one family or one therapy. It exposes how Europe’s fragmented genomic medicine ecosystem, at both European and national levels, causes delays, duplication, and uncertainty. EGMEDC was created to address precisely these gaps: by bringing patient groups together with clinicians, translational scientists, regulators, industry partners, and policymakers, and by turning dialogue into practical, repeatable pathways rather than isolated exceptions.
Rare diseases are often treated as isolated cases, yet together they affect an estimated 27–36 million people across Europe. The challenge with ultra-rare conditions is not only low prevalence, but economics. Genomic medicines are costly to develop, and when each therapy serves only a handful of patients, those costs appear disproportionate. Regulation compounds this problem. Even when therapies rely on validated delivery platforms, closely related treatment variants are often regulated as entirely new products. A platform-based approach, paired with clearly defined clinical freedom to operate within standardized protocols, could reduce duplication while preserving patient safety.
This same platform logic also changes the cost equation. When one therapeutic framework can serve multiple related disorders, ‘ultra-rare’ becomes more common. Earlier intervention in severe, progressive diseases can prevent decades of supportive care. From this perspective, the real question is not whether healthcare systems can afford to invest in innovation, but why they so rarely do, despite the potential for better outcomes and lower long-term costs.
Some countries have begun to experiment with alternative models. In the Netherlands and Germany, insurers and public systems have supported evidence generation alongside care. 3, 4 These efforts remain exceptions, but they do point to what is possible.
For EGMEDC, the direction is clear: safeguard safety, reduce unnecessary repetition, align standards, and make cross-border access a supported pathway instead of a personal struggle. If Europe can move faster for patients like August, it can establish a genomic medicine model that delivers timely care and fully reap the benefits of already established scientific excellence.
Text by Laura Roy and Henri van de Vrugt, New Haven Biosciences Consulting, For more information contact: henri@crisprmedicinenews.com
Disclosure of potential conflicts of interest:
HvdV is a freelance writer for CRISPR Medicine News and independent advisor to the European Genomic Medicine Consortium. He is a founding partner of New Haven Biosciences Consulting, Connecticut, and CEO of Bio Avenues, Utrecht, the Netherlands. LR is a founding partner of New Haven Biosciences Consulting.