Aldevron Joins EGMEDC to Turn Genomic Promise Into...
May. 6, 2026

CMN Intelligence - The World’s Most Comprehensive Intelligence Platform for CRISPR-Genomic Medicine and Gene-Editing Clinical Development
Providing market intelligence, data infrastructure, analytics, and reporting services for the global gene-editing sector. Read more...
(Interview is condensed and edited for clarity)
- Hi Mandy and Jan, thanks for taking the time to speak with me. Can you start by telling me a bit about the haemoglobinopathies Ariya Bio will focus on?
Jan: The two haemoglobinopathies that we are most interested in are sickle cell disease (SCD) and beta thalassemia (BT). These are the most common monogenetic disorders worldwide, with approximately 7% of the world population being a carrier for one of these diseases. This roughly translates into 6 million patients globally.
Symptoms can vary greatly between individual patients, and these diseases exist along a continuum of severity, with fatigue or anaemia in the mild end, and severe anaemia and multi-organ damage in the severe end. About half of all patients with HbSS, which is a severe sub-form of SCD whereby patients inherit genes encoding the diseased haemoglobin variant haemoglobin “S” from both parents, die before they turn 45.
- And how does the current treatment landscape look for these diseases?
Mandy: Despite their prevalence, treatments for both diseases are still quite limited. There is one approved viral-based gene therapy in the US for transfusion-dependent BT, Zynteglo (developed by bluebird bio), but this has faced concerns as some patients treated with similar viral-based vectors developed blood cancer.
As of right now, there is no safe, effective, and readily available cure for SCD or BT. Until new therapies are developed, the only potential curative option for patients is stem cell transplantation from a genetically-matched donor, but this strategy is heavily limited by donor availability, and even with a matched donor, stem cell transplants face quite a high risk of failure.
The β-haemoglobinopathies, which include sickle cell disease and β-thalassemia, are among the most prevalent inherited disorders worldwide and arise through mutations that impact the structure or production of the β-globin subunits found in adult haemoglobin A1 (HbA1).
A number of gene-editing strategies that either centre around correcting β-globin mutations or reactivating foetal haemoglobin expression have progressed to ongoing clinical trials. Meanwhile, δ-globin, which is the subunit of the less abundant form of adult haemoglobin, HbA2, remains a relatively unexplored therapeutic target for β-haemoglobinopathies.
Recognising that δ-globin demonstrates high homology to β-globin and is already pan-cellularly expressed at low levels in adult red blood cells, the team that would become Ariya Bio investigated whether CRISPR-Cas9-mediated correction of non-functional transcriptional elements in the endogenous δ-globin promoter would elevate overall expression of HbA2.
They found that CRISPR-mediated restoration of three specific transcription factor elements (KLF1, β-DRF, and TFIIB) led to robust upregulation of the δ-globin-expressing gene HBD from the endogenous locus in clonal populations of a human erythroid progenitor cell line as well as primary erythroblasts. The increase in HBD expression coincided with elevated HbA2 levels in excess of 10x-fold greater than wild-type unedited cells. The full study details and findings were recently published in eLife (Boontanrart et al., 2023).
Mandy Y Boontanrart, Elia Mächler, Simone Ponta, Jan C Nelis, Viviana G Preiano, Jacob E Corn (2023) Engineering of the endogenous HBD promoter increases HbA2 eLife 12:e85258.
- Which gene-editing reagents are you using and what is your chosen delivery strategy?
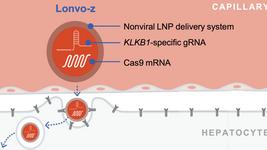
Jan: While our therapeutic strategy is novel, our gene-editing approach is similar to what others are doing from a protocol point of view. We are using Cas9 ribonucleoprotein and single guide RNAs to target the locus of interest (in this case the HBD promoter), which are delivered to cells via electroporation. We add single-stranded oligodeoxynucleotides (ssODNs) as the donor template; this allows us to insert the motifs mentioned earlier. In a therapeutic setting, all those reagents would be delivered to a patient’s own blood stem cells ex vivo via electroporation, and the edited cells would then be transplanted back into the patient’s bone marrow.
Mandy: Although we have chosen to focus on ex vivo patient-derived stem cell editing at present, our therapeutic mechanism is not restricted to an ex vivo approach, and we may explore in vivo promoting-editing strategies in the future.
- There are some ongoing attempts to develop therapies that correct the single disease-causing mutation in SCD. Such treatments should eliminate defective HbA1 from patient blood. What happens to the defective HbA1, in SCD, when you upregulate HbA2?
Mandy: Based on our data so far, we don’t believe that our approach to upregulate HbA2 leads to downregulation of β-globin, so HbA1 would still be present even with increased HbA2, but this shouldn’t be a major concern. The SCD mutation causes the defective haemoglobin molecules to polymerise, but studies have shown that expression of beneficial haemoglobins (such as HbA2) should prevent this, if there is enough HbA2 present.
As a side note, we are aware that others are developing therapies that target the underlying mutation in SCD. This is obviously an attractive approach for SCD, but since beta-thalassemia is caused by any of several hundred mutations in the HBB gene, any therapy to fix the root cause of disease would require a separate development programme for every type of mutation. With our approach, we can address both patient groups and potentially treat many more patients with a single therapy.
Video description: Using CRISPR-Cas9 to repair the HBD promoter leads to increased production of hemoglobin HbA2. This video illustrates the promoter-editing strategy developed by researchers in the Corn Lab at ETHZ (https://www.cornlab.com). The team used CRISPR-Cas9 to edit transcriptional elements in the HBD promoter, which upregulates the expression of adult haemoglobin A2. The researchers are now exploring this approach as a new way to treat β-hemoglobinopathies.
Co-founder, Jan Nelis will speak at the upcoming CRISPR Medicine Conference, Copenhagen, Denmark April 23-25 2024.
- Do you believe that HbA2 is superior to foetal haemoglobin from a therapeutic point of view?
Mandy: Yes, we believe that HbA2 is a better target for several reasons. Firstly, it is more similar in structure and function to adult haemoglobin, with 93 % sequence homology between the two, compared to foetal haemoglobin, which only shares 76 % homology with HbA1. In addition, from a functional standpoint, foetal haemoglobin has elevated oxygen affinity compared to the adult haemoglobins, and the potential implications of persistently high levels of foetal haemoglobin on human physiology, in particular during pregnancy, are not yet clear.
Jan: The high levels of foetal haemoglobin that are achieved in the ongoing development programmes are not widely observed in nature. In contrast, HbA2 is already expressed in all adult red blood cells, albeit in small amounts, which suggests that it should be safe to express. Another interesting fact here is that HbA2 is actually the predominant form of haemoglobin in some species, such as dogs, which indicates that high levels of HbA2 are safe in mammals.
- So how and when did Ariya Bio get started?
Mandy: It really started with a fundamental question about how HbA2 was regulated. We were not thinking about developing a therapy at all in the beginning, but rather looking at genetic regulation of HbA2 and trying to figure out why two types of haemoglobin exist in adults, and why one of them is so lowly expressed.
Although we only started working on Ariya Bio quite recently, I began my PhD in 2015 and my dissertation was on the genetic regulation of haemoglobins. Jan and I started working together in 2021. During my PhD, I was looking closely at the promoters of the various haemoglobin genes and noticed that quite a few transcription factor elements were missing in HBD, whose protein product is required for the δ-globin subunits in HbA2. Other groups have reported transgenic approaches to replace these elements by inserting a KLF1 motif in the HBD promoter, but we were the first to show that CRISPR-mediated insertion of KLF1, β-DRF, and TFIIB motifs into the endogenous HBD promoter can lead to a 10-fold upregulation in HbA2 expression in various cell types. These results were very exciting and highlighted to us the therapeutic potential of upregulating HbA2 to treat haemoglobinopathies. No one else was doing it, so we started Ariya Bio to translate our scientific discoveries into a new therapy.
- I know it’s early days, but what can you share about Ariya’s pipeline so far?
Jan: Our lead programmes are focused on the HbA2-upregulating strategy we’ve discussed here, for two indications: severe SCD and transfusion-dependent BT.
We are currently at the pre-clinical stage with both programmes, with a plan to advance ARY001 and ARY002 to the clinic for SCD and BT, respectively. We are still optimising the gene-editing reagents, and we plan to start in vivo engraftment studies before the end of 2023. These studies are crucial, as they will test how effectively CRISPR-edited patient-derived cells can engraft and express HbA2. They will likely run for a few months, and hopefully after that point we can begin to compile the data needed to submit an investigational new drug (IND) or clinical trial application (CTA) towards the middle or end of 2024.
Jan: Regarding clinical development, we are open for several scenarios including co-development with a partner, and we have already initiated talks with suitable industry partners. We are also in the very early stages of exploring whether we can adapt our promoter-editing strategy to other indications. We can’t say more about which diseases we are looking at, but we are very excited about how far we can go with our novel approach.
- Thanks to you both for speaking with me. We look forward to future developments from Ariya Bio!
Disease Roundup: Four Gene-Editing Candidates in the Clinic for Sickle Cell Disease
Clinical Roundup: Gene-Edited Therapies for Beta Thalassemia
ArticleInterviewNewsBeta ThalassemiaSickle Cell Disease, SCDBlood diseaseCas9ARIYA BIO